Standard tests for vitamins and minerals by A/Prof Ken Sikaris BSc (Hons), MBBS, FRCPA, FAACB, FFSc
 Anthea Talliopoulos, APD
Anthea Talliopoulos, APD
Interpreting vitamin and mineral tests can be challenging, and in requesting tests as dietitians, it is important that we can justify the reason for testing. It is also crucial that in interpreting laboratory results and interpreting biochemical markers that we can alter our dietary plan and/or alter the supplement regimens of our patients in a safe manner.
In this very informative and practical presentation, Chemical Pathologist Associate Professor Ken Sikaris shares his knowledge and expertise to talk us through the interpretation of vitamin and mineral testing through real-life case studies.
Points to keep in mind when recommending and/or interpreting mineral testing:
- Chromium is very difficult to measure, although whole blood chromium is a better indicator of actual stores than serum chromium.
- Thyroid testing can be used an indicator of iodine stores, rather than iodine testing in isolation.
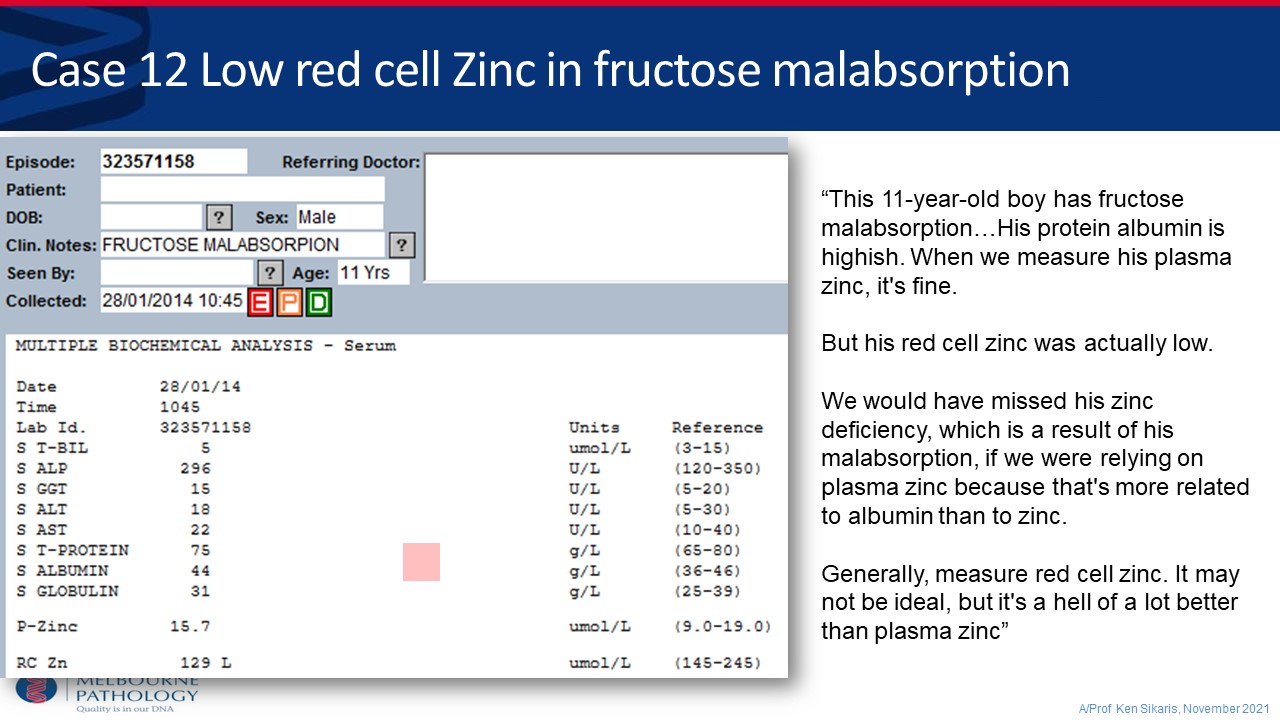
- Measuring red blood cell zinc as opposed to plasma zinc should be more widely encouraged as this a much more accurate measure as actual stores.
- Remember that in a state of acute inflammation with elevated CRP, albumin can be falsely low, as well as zinc (as zinc is bound to albumin in the bloodstream). This means that measuring zinc levels in acutely unwell patients, such as in a hospital setting, we will likely get a falsely low level.
- Similarly to zinc being bound to albumin, copper is bound to ceruloplasmin; thus, in measuring copper, we are mainly measuring ceruloplasmin. Ceruloplasmin increases in inflammation, making copper levels even harder to assess when CRP is elevated.
Key points regarding interpretation of vitamin tests which he shares in this presentation include:
- It is critical that in assessing fat soluble vitamin levels, such as vitamins A and E, that we also closely monitor blood lipids. This is due to fat soluble vitamins being carried via lipoproteins.
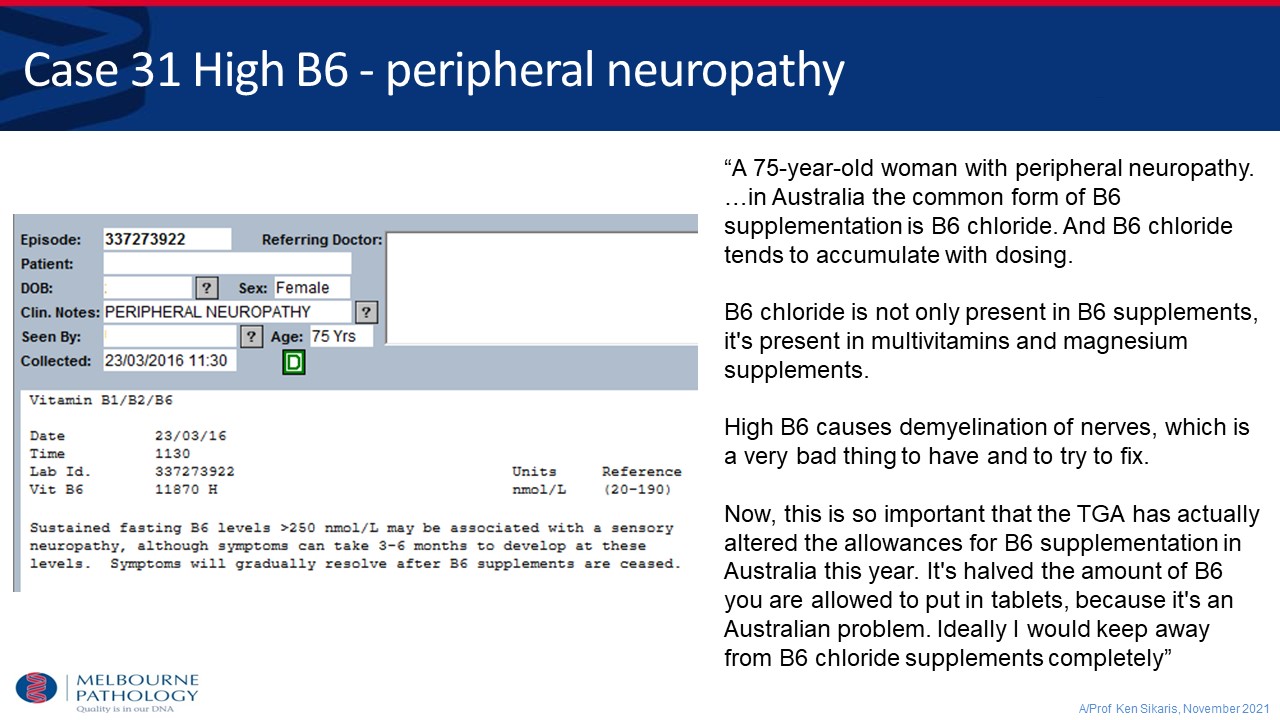
- Vitamin B6 has a direct impact on ALT and AST levels; thus, if vitamin B6 levels are low, we can expect to see lower levels of ALT and AST when assessing LFTs.
- Caution should be exercised in recommending supplements containing vitamin B6 (especially B6 hydrochloride) as excessive B6 is an emerging issue in Australia and has been linked to demyelination of nerves.
- Folate deficiency is extremely rare in Australia since mandatory fortification procedures were introduced and does not need to be routinely tested for in healthy individuals.
- Vitamin B12 status can be assessed through total B12, except in cases such as pregnancy in which holotranscobalamin is a more accurate measure. If B12 is low, iron should always be checked, especially in higher risk groups, such as those following a vegan diet.
As clinicians, we should continue to exercise caution in supplementing vitamins and minerals, always ensuring that there is a clinical basis as inappropriate supplementation can be harmful.
To register for the presentation and associated documents including the assessment quiz click here